

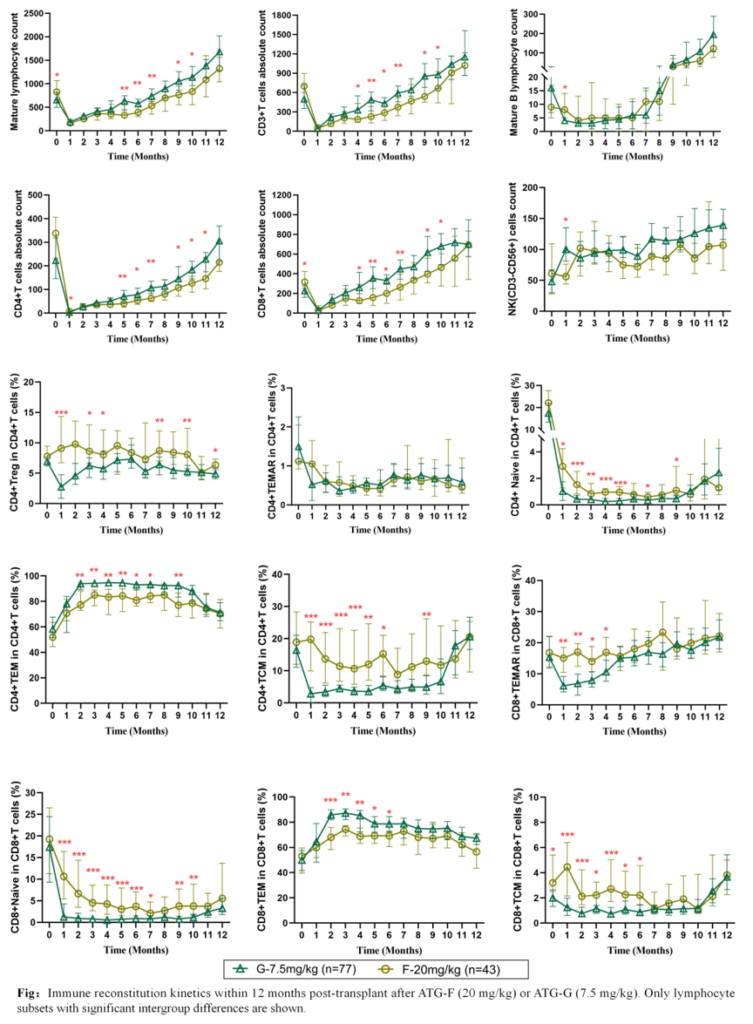
The 2026 Congress of the European Hematology Association (EHA 2026), held from June 11–14 in Stockholm, Sweden, brought together leading experts from around the world to showcase the latest advances in hematology research, translational medicine, and clinical practice.Among the studies presented at this year’s meeting was an important investigation led by Hui Wang and Man Chen from Lu Daopei Hospital, examining the impact of two commonly used antithymocyte globulin (ATG)-based conditioning regimens on immune reconstitution following allogeneic hematopoietic stem cell transplantation (allo-HSCT).
The study revealed distinct patterns of immune recovery associated with the two regimens. While the ATLG-based approach was associated with slower T-cell numerical recovery, it preserved greater immune diversity, promoted earlier and more sustained regulatory T-cell (Treg) reconstitution, and appeared to support a more tolerant immune environment. These findings provide valuable immunological insights for optimizing conditioning strategies and highlight the importance of considering both the quantity and quality of immune reconstitution after transplantation.
Study Overview
Title: Effects of Two Antithymocyte Globulin Conditioning Regimens on Immune Reconstitution after Allogeneic Hematopoietic Stem Cell Transplantation
First Author: Man Chen Corresponding Author: Hui Wang
Background
Allogeneic hematopoietic stem cell transplantation remains a potentially curative treatment for a variety of hematologic malignancies. However, long-term outcomes are heavily influenced by the quality of post-transplant immune reconstitution, which affects infection risk, relapse control, overall survival, and the development of graft-versus-host disease (GVHD).
Antithymocyte globulin is widely incorporated into conditioning regimens to reduce GVHD risk. Despite its routine use, the long-term effects of different ATG formulations and dosing strategies on immune recovery remain incompletely understood.
Two of the most commonly used approaches are:
- Rabbit anti-human thymocyte immunoglobulin (rATG, 7.5 mg/kg)
- Rabbit anti-human T-lymphocyte immunoglobulin (ATLG, 20 mg/kg)
Given their distinct pharmacologic properties and dosing schedules, determining which regimen better supports durable, tolerant, and leukemia-controlling immune reconstitution remains an important clinical question.
Methods
The study included 120 patients who underwent allo-HSCT.
Seventy-seven patients received rATG at 7.5 mg/kg, while 43 patients received ATLG at 20 mg/kg.
Peripheral blood lymphocyte subsets were monitored before transplantation and throughout the first 12 months after transplant. Analyses included:
- Total lymphocyte counts
- CD3⁺ T cells
- CD4⁺ T cells
- CD8⁺ T cells
- B cells
- NK cells
- NKT cells
The investigators also performed detailed phenotypic analyses of T-cell subsets, including:
- Naïve T cells
- Central memory T cells (TCM)
- Effector memory T cells (TEM)
- Terminally differentiated T cells
- Regulatory T cells (Tregs)
Baseline clinical characteristics, GVHD incidence, engraftment kinetics, and viral reactivation data were also compared between the two groups.
Results
Baseline characteristics were generally well balanced between the two cohorts. No significant differences were observed with respect to age, sex, infused cell dose, engraftment timing, disease duration, or timing of viral reactivation.
The incidence of Grade III–IV acute GVHD was similar between the two groups. Although moderate-to-severe chronic GVHD occurred more frequently in the rATG group (15.6%) than in the ATLG group (7.0%), this difference did not reach statistical significance.
One notable limitation was the imbalance in conditioning regimens. Most patients in the rATG cohort received busulfan/cyclophosphamide (BU/CY), whereas a substantially higher proportion of patients in the ATLG cohort received total body irradiation/cyclophosphamide (TBI/CY).
Two Distinct Patterns of Immune Reconstitution
The investigators observed markedly different immune recovery trajectories between the two treatment groups.
Faster Quantitative T-Cell Recovery with rATG
Patients receiving rATG experienced more rapid expansion of total T-cell populations after transplantation.
Beginning approximately four months after transplant, CD4⁺ and CD8⁺ T-cell counts were consistently higher in the rATG group compared with the ATLG group. These differences remained significant at multiple time points throughout follow-up.
From a purely numerical perspective, rATG appeared to facilitate faster immune reconstitution.
Greater Immune Diversity and Reserve with ATLG
Although T-cell counts recovered more slowly in the ATLG group, the composition of the T-cell repertoire differed substantially.
Patients treated with ATLG demonstrated significantly higher proportions of:
- Naïve CD4⁺ T cells
- Central memory CD4⁺ T cells
These differences were evident during the first several months following transplantation.
In contrast, the rATG group exhibited a predominance of effector memory T cells, with CD4⁺ TEM populations exceeding 90% at several time points.
According to the investigators, the higher proportions of naïve and central memory T cells observed in the ATLG group suggest greater immunologic reserve and broader immune diversity, characteristics generally associated with more adaptable long-term immune recovery.
Earlier and More Durable Treg Reconstitution with ATLG
One of the most striking findings involved regulatory T cells.
The ATLG regimen consistently promoted superior Treg recovery compared with rATG.
The proportion of CD4⁺ Tregs among total CD4⁺ T cells was significantly higher in the ATLG group at multiple time points, including months 1, 3, and 12 after transplantation.
Importantly, this advantage emerged early and persisted over time.
Because Tregs play a central role in maintaining immune tolerance and suppressing alloreactivity, the investigators suggest that enhanced Treg reconstitution may contribute to the lower observed tendency toward chronic GVHD in the ATLG cohort.
Clinical Implications
The findings indicate that the two conditioning strategies produce fundamentally different patterns of immune reconstitution.
The rATG regimen is characterized by rapid numerical recovery of T cells, particularly effector memory populations. While this may accelerate immune restoration, it is accompanied by delayed Treg recovery and a less diverse T-cell repertoire.
By contrast, the ATLG regimen supports a slower but potentially more balanced immune recovery process. Preservation of naïve and central memory T-cell populations, together with earlier and more sustained Treg reconstitution, may promote a more tolerant and immunologically resilient post-transplant environment.
These observations suggest that successful immune reconstitution should not be judged solely by cell counts. The quality, diversity, and functional composition of the recovering immune system may be equally important determinants of long-term outcomes.
Conclusion
This study provides important evidence that different ATG-based conditioning strategies can profoundly influence the trajectory of immune recovery following allo-HSCT.
While rATG 7.5 mg/kg promotes more rapid T-cell expansion, ATLG 20 mg/kg appears to preserve greater immune diversity and facilitate earlier, more durable Treg recovery. This pattern may contribute to improved immune tolerance and a lower tendency toward chronic GVHD.
The investigators emphasize that the unequal distribution of conditioning regimens between groups, particularly the differing use of TBI-based conditioning, may have influenced some findings. Additional studies will therefore be needed to clarify the independent effects of ATLG and rATG on immune reconstitution.
Nevertheless, the results highlight an important principle in transplantation medicine: optimal immune recovery requires not only quantitative reconstitution but also qualitative restoration of a diverse and well-regulated immune system.
Expert Profiles
Hui Wang
Lu Daopei Hospital
Vice President, Beijing Lu Daopei Institute of Hematology Deputy Director (Vice President Level), Department of Clinical Laboratory, Lu Daopei Hospital
Professor Wang has more than 24 years of experience in flow cytometry and laboratory diagnostics and has independently reviewed over one million clinical laboratory reports.
She serves on the editorial boards of the Chinese Journal of Laboratory Medicine and the Chinese Journal of Hematology and holds leadership positions in more than 20 national academic organizations related to laboratory medicine, flow cytometry, hematology, and oncology.
Professor Wang holds 10 Chinese invention patents and three U.S. patents. She has led the development of six expert consensus statements and contributed to numerous additional clinical guidelines and standards. As first author or corresponding author, she has published more than 60 SCI-indexed and core Chinese journal articles.
Man Chen
Lu Daopei Hospital
Supervisor, Flow Cytometry Laboratory Associate Chief Medical Technologist / Associate Physician
Academic Appointments
- Committee Member, Fourth Laboratory Medicine Committee, Beijing Association of Integrative Medicine
- Member, Clinical Flow Cytometry Working Group, Chinese Medical Doctor Association
- Youth Committee Member, Chinese Association of Integrative Medicine Laboratory Committee
- Standing Committee Member and Secretary, Flow Cytometric Analysis and Diagnostic Expert Committee, Chinese Association of Integrative Medicine
- Standing Committee Member, Flow Cytometry Group, China Quality Assurance Program (CQAP) Laboratory Medicine Committee
- Standing Committee Member, Cytokine and Disease Detection Group, Bethune Spirit Research Society
- Member, Expert Committee of the Beijing Economic-Technological Development Area Laboratory Quality Control and Improvement Center
Professional Achievements
Ms. Chen has worked in flow cytometry diagnostics and laboratory medicine for more than 14 years and is responsible for maintaining College of American Pathologists (CAP) accreditation for the flow cytometry laboratory.
She has received the Beijing Yizhuang Outstanding Talent Award and has won two Hebei Medical Science and Technology Awards. As first author or corresponding author, she has published 24 SCI-indexed and core journal articles.
She is the primary inventor on one Chinese invention patent and co-inventor on six additional Chinese patents and three U.S. patents. She has contributed to nine national expert consensus statements in flow cytometry, served as lead writer for two of them, and participated in the development of two national flow cytometry standards.

