

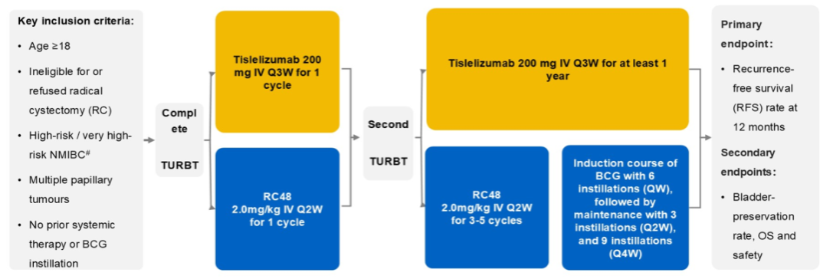
Transurethral resection of bladder tumor (TURBT) remains the standard treatment for non-muscle-invasive bladder cancer (NMIBC). However, up to 45% of patients experience tumor recurrence within one year following TURBT alone. Although intravesical therapies—including cytotoxic agents and immunotherapy—are widely used, substantial unmet clinical needs remain, underscoring the need for more effective treatment strategies. The PUNCH03 study, led by Prof. Junxing Chen from The First Affiliated Hospital of Sun Yat-sen University, investigated disitamab vedotin combined with Bacillus Calmette-Guérin (BCG) for patients with high-risk NMIBC. The regimen not only reduced residual disease and recurrence risk but also offered new hope for bladder preservation. The study was selected for presentation at the 2026 American Society of Clinical Oncology (ASCO) Annual Meeting, highlighting international recognition of this innovative Chinese approach.
Oncology Frontier–UroStream invited Prof. Junxing Chen to discuss the study findings and their clinical significance for improving the management of high-risk NMIBC in China.
Oncology Frontier–UroStream
Patients with high-risk NMIBC continue to face the dual challenges of bladder preservation and high recurrence rates, particularly those with multiple papillary tumors that are difficult to resect completely. Your PUNCH03 study was presented at this year’s ASCO meeting, showcasing a Chinese treatment strategy to the global community. How does the disitamab vedotin–based combination address these major clinical challenges?
Prof. Junxing Chen
In recent years, bladder-preserving treatment strategies for muscle-invasive bladder cancer (MIBC) have become a major focus of clinical research. Meanwhile, bladder preservation for patients with high-risk NMIBC remains particularly challenging.
Intravesical BCG has long been the cornerstone of treatment. However, with the remarkable success of immunotherapy and targeted therapy in advanced urothelial carcinoma, increasing efforts are being made to move these therapies into earlier disease settings.
In daily clinical practice, patients with multiple papillary tumors often present significant surgical challenges because complete tumor resection is difficult to achieve. Consequently, many ultimately undergo radical cystectomy. Against this backdrop, introducing a targeted immunotherapy strategy such as disitamab vedotin earlier in the treatment course may create new opportunities for bladder preservation in patients who previously had limited options.
For these patients, we employed a disitamab vedotin–based targeted combination regimen, followed by intravesical BCG as consolidation therapy. This intensified multimodal strategy represents an innovative approach for high-risk NMIBC and offers renewed hope for bladder preservation.
As larger clinical studies continue to mature, we believe that targeted combination therapy will enable an increasing number of patients with high-risk NMIBC to preserve their bladder while maintaining effective disease control.
Oncology Frontier–UroStream
The PUNCH03 regimen not only reduced recurrence risk but also introduced new possibilities for bladder preservation. Could you share the key study results and explain their clinical significance for Chinese patients with high-risk NMIBC?
Prof. Junxing Chen
PUNCH03 is a single-center study. As of the data cutoff in August 2025, 24 patients had been evaluated.
Most participants were male (87.5%), with a median age of 63 years. HER2 expression by immunohistochemistry was 2+ in 58.3% and 3+ in 41.7% of patients. Additionally, 75% presented with multiple papillary tumors, reflecting the characteristics of high-risk NMIBC commonly encountered in real-world Chinese clinical practice.
The study demonstrated a 12-month bladder preservation rate of 95.8%. Only two patients experienced recurrence, and one patient ultimately underwent radical cystectomy.
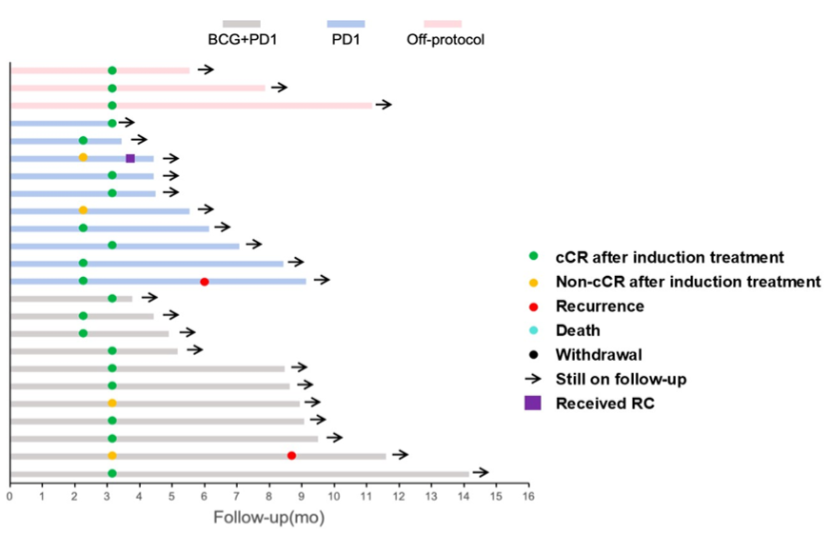
Importantly, no Grade 3–5 treatment-related adverse events were observed. These findings indicate that the study successfully achieved its predefined objectives and provide a promising new treatment strategy for Chinese patients with high-risk NMIBC.
Among patients with HER2-overexpressing high-risk NMIBC, additional encouraging efficacy was observed.
In Cohort A (adjuvant disitamab vedotin monotherapy; n=22), the 6-month and 12-month recurrence-free survival (RFS) rates were 95.2% and 73.4%, respectively.
In Cohort B (salvage therapy following BCG failure; n=6), the 3-month complete clinical response rate reached 100%, while the median duration of response had not yet been reached.
Exploratory analyses further showed that patients with positive baseline urinary tumor DNA (utDNA) had significantly lower 1-year recurrence-free survival than those with negative utDNA (50% vs. 91%; P=0.043).
Overall, these preliminary findings suggest that this innovative treatment strategy may open a new pathway for bladder preservation while improving quality of life for patients with high-risk NMIBC.
Oncology Frontier–UroStream
Your study adopted an innovative strategy of targeted combination therapy followed by BCG induction. Mechanistically, how does HER2-targeted drug delivery alter the tumor microenvironment or reduce tumor burden to improve subsequent induction therapy and facilitate bladder preservation?
Prof. Junxing Chen
Current evidence from both laboratory and clinical studies consistently indicates that HER2 overexpression is associated with poor prognosis in urothelial carcinoma.
Studies have demonstrated that patients with HER2-overexpressing NMIBC have a substantially higher risk of progression to MIBC than HER2-negative patients. HER2 overexpression is therefore considered a marker of aggressive tumor biology and poor clinical outcomes.
In clinical practice, we have also observed that patients with high HER2 expression often respond poorly to intravesical BCG therapy. Fortunately, HER2 represents an ideal therapeutic target for antibody-drug conjugates (ADCs).
Based on this rationale, we developed a novel treatment strategy. Disitamab vedotin is first administered to selectively eliminate HER2-positive tumor cells, after which BCG instillation is introduced to consolidate treatment. This sequential approach creates a synergistic therapeutic effect.
The strategy not only enhances treatment efficacy but also provides a new option for patients who previously failed BCG therapy, creating additional opportunities for successful bladder preservation in high-risk NMIBC.
Oncology Frontier–UroStream
Your study, together with recent international research on ctDNA and other biomarkers, points toward more precise treatment selection in urothelial carcinoma. Based on PUNCH03 and related analyses, how do you view the potential of HER2 expression, ctDNA, and other biomarkers in guiding bladder-preserving treatment for NMIBC?
Prof. Junxing Chen
One of the greatest challenges clinicians face today is identifying the patients most likely to benefit from a given treatment.
We still need better methods to determine which patients are most responsive to immunotherapy, which are more likely to benefit from targeted therapy, and which are resistant to immune-based treatment. At present, no biomarker has yet entered routine clinical practice with sufficient maturity to reliably guide precision treatment.
Nevertheless, biomarker research continues to advance rapidly. Studies evaluating HER2 expression, circulating tumor DNA (ctDNA), and urinary tumor DNA (utDNA) are generating increasingly valuable evidence.
HER2 overexpression has already been established as an adverse prognostic factor in both MIBC and advanced urothelial carcinoma, and it also independently predicts poor response to BCG therapy in patients with high-risk NMIBC. Targeting HER2 therefore has considerable potential to improve treatment outcomes.
Meanwhile, ctDNA may reflect the long-term persistence of tumor cells throughout the body, whereas utDNA provides valuable information regarding residual local disease. These liquid biopsy–based biomarkers offer powerful tools for precision patient selection, enabling clinicians to tailor treatment more effectively.
Ultimately, ctDNA and utDNA testing may help determine whether patients are better suited to systemic therapy or intensified local treatment, facilitating increasingly personalized treatment strategies.
Oncology Frontier–UroStream
Disitamab vedotin–based regimens have already been approved for first-, second-, and later-line treatment of advanced urothelial carcinoma. You and other investigators have also explored its use in NMIBC and MIBC, expanding bladder-preserving options. How do you view its role in the overall management of urothelial carcinoma, and what additional studies are needed to strengthen the evidence base?
Prof. Junxing Chen
Traditionally, bladder-preserving treatment has followed a classic “sandwich” model centered on maximal TURBT combined with concurrent chemoradiotherapy.
With the emergence of targeted therapy and immunotherapy, however, we and many colleagues across China have begun exploring a new triplet treatment strategy focused on comprehensive perioperative management.
This approach begins with individualized neoadjuvant therapy, using disitamab vedotin, immunotherapy, or chemo-immunotherapy according to each patient’s disease characteristics. Surgery is then performed, followed by tailored postoperative adjuvant therapy.
This modern “sandwich” strategy integrates neoadjuvant treatment, surgery, and postoperative therapy into a comprehensive treatment framework that has the potential to reshape the management of both NMIBC and MIBC.
As more innovative therapies become available, long-term management of bladder cancer presents new challenges, including optimizing efficacy while monitoring long-term toxicity. These issues have become central to perioperative bladder cancer management.
Based on this innovative treatment model, we believe that more patients will achieve improved outcomes, preserve their bladder, and ultimately enjoy better long-term survival.
Expert Profile

Prof. Junxing Chen
The First Affiliated Hospital of Sun Yat-sen University
