Urothelial carcinoma is one of the most common malignancies of the urinary tract, with bladder cancer representing its most prevalent subtype. In recent years, immunotherapy has offered new hope for patients with advanced disease. However, not all patients derive meaningful benefit.
Why are some tumors intrinsically resistant to immunotherapy? What biological mechanisms determine treatment response?
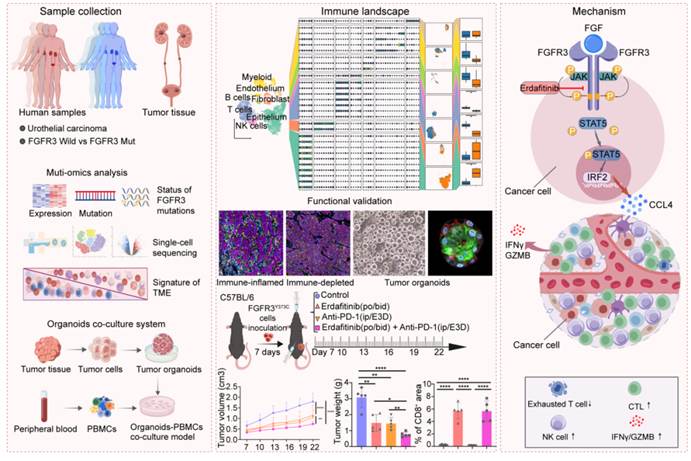
To address these questions, Professor Tao Xu’s team from the Department of Urology at Peking University People’s Hospital, in collaboration with Professor Yihan Lin’s team from the Center for Quantitative Biology at Peking University, investigated the mechanisms underlying immunotherapy resistance in urothelial carcinoma. Using patient-derived tumor samples, organoid models, immune co-culture systems, and multi-omics technologies, the researchers uncovered key drivers of immune resistance and identified potential strategies for precision combination therapy.
Recently, the study was published online in the international journal iMeta.
The research focused on one of the most pressing clinical challenges in urothelial carcinoma: resistance to immune checkpoint inhibitors. By establishing an innovative patient-derived organoid–immune cell co-culture platform and integrating single-cell RNA sequencing, whole-exome sequencing, epigenomic profiling, and other multi-omics approaches, the investigators systematically dissected the mechanisms through which FGFR3-mutant urothelial carcinoma develops an immunosuppressive tumor microenvironment.
Their findings support a novel therapeutic strategy combining targeted therapy with immunotherapy and provide important experimental evidence for precision treatment of advanced urothelial carcinoma.
Addressing a Critical Clinical Challenge: Why Does Immunotherapy Resistance Occur?
In recent years, immune checkpoint inhibitors targeting the PD-1/PD-L1 pathway have expanded treatment options for patients with advanced urothelial carcinoma. Nevertheless, a substantial proportion of patients experience limited benefit or eventually develop resistance, creating a major barrier to further improving clinical outcomes.
The effectiveness of immunotherapy is closely linked to the tumor microenvironment. If antitumor immune cells—including T cells and natural killer (NK) cells—cannot efficiently infiltrate tumor tissue, or if they lose their cytotoxic function after entering the tumor, the cancer may develop an “immune desert” or “cold tumor” phenotype, rendering immunotherapy less effective.
To investigate this challenge, the research team focused on FGFR3 mutations, one of the most common genetic alterations in urothelial carcinoma, and explored how these mutations influence the tumor immune microenvironment and contribute to immunotherapy resistance.
An Innovative Research Platform: Using Organoid–Immune Co-Culture Models to Reveal Resistance Mechanisms
To more accurately replicate patient biology, the investigators established a patient-derived urothelial carcinoma organoid–immune co-culture system (UCOs-PBMCs).
Organoids are three-dimensional structures grown from patient tumor tissue that preserve many of the original tumor’s genetic features and biological heterogeneity.
The team further co-cultured urothelial carcinoma organoids with patients’ peripheral blood mononuclear cells (PBMCs), creating a platform that mimics the dynamic interactions between tumor cells and immune cells.
Using this model in combination with:
- Single-cell RNA sequencing
- Whole-exome sequencing
- Epigenomic profiling
- Multi-omics integration
the researchers systematically analyzed resistance mechanisms across multiple biological dimensions, including genomic alterations, immune-cell composition, cellular states, and regulatory networks.
FGFR3 Mutations Drive the Formation of an Immunosuppressive Tumor Microenvironment
The study identified FGFR3 mutation as a major driver of immune suppression in urothelial carcinoma.
In FGFR3-mutant tumors, investigators observed:
- Significant reductions in NK cells
- Significant reductions in CD8⁺ cytotoxic T cells
- Enrichment of terminally exhausted T-cell populations
These findings indicate profound suppression of local antitumor immune responses.
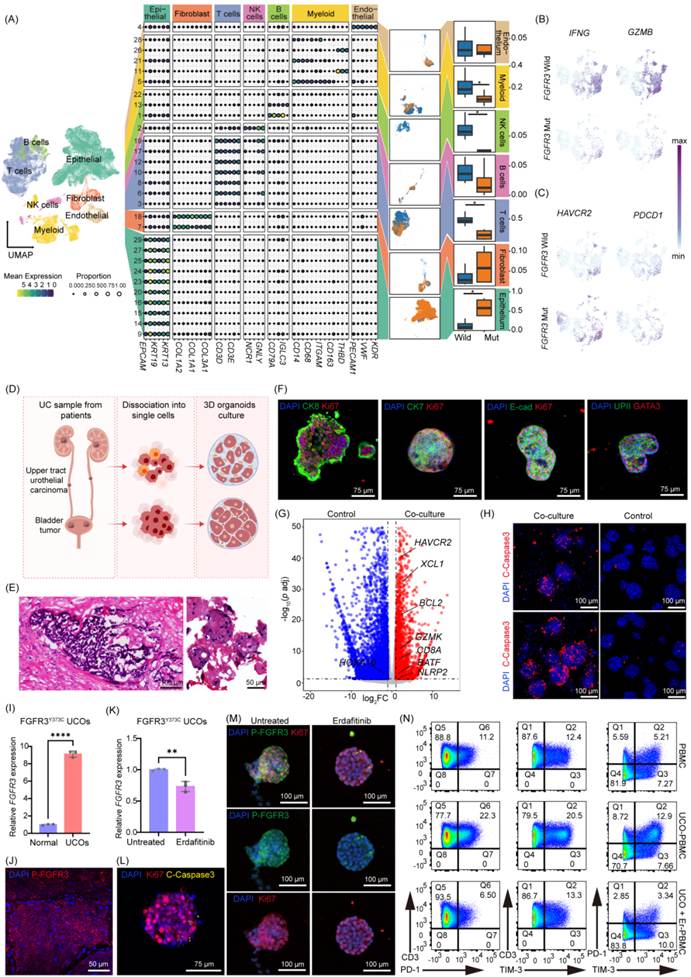
Further mechanistic investigations revealed that aberrant FGFR3 activation suppresses expression of the chemokine CCL4 through the downstream STAT5–IRF2 signaling pathway.
CCL4 plays a critical role in recruiting immune cells into tumor tissue. When CCL4 expression is inhibited:
- NK-cell infiltration decreases
- CD8⁺ T-cell infiltration decreases
- Antitumor immune surveillance is impaired
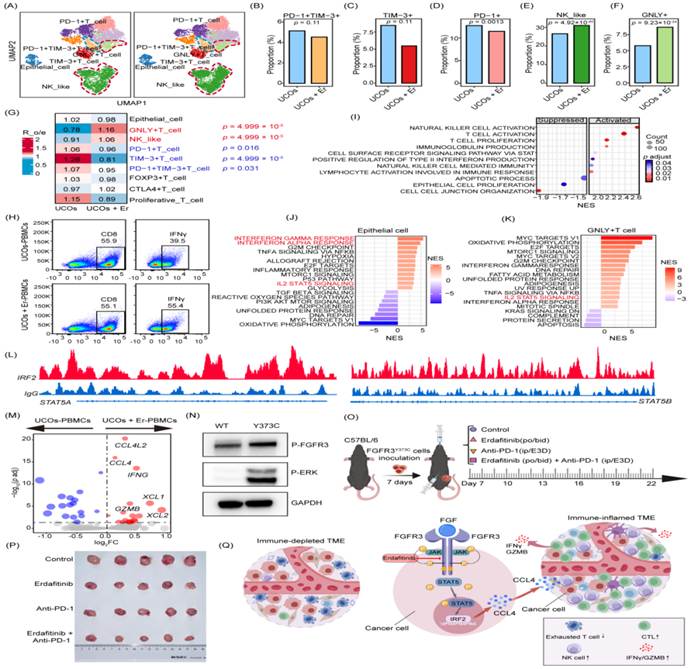
As a result, tumors develop an “immune desert” microenvironment that limits the effectiveness of immune checkpoint blockade.
This work identifies the FGFR3–STAT5–IRF2 signaling axis as a key regulator of immunotherapy resistance in urothelial carcinoma and provides new mechanistic insight into why FGFR3-mutant tumors often exhibit poor sensitivity to immunotherapy.
Translational Implications: A New Rationale for Combining Targeted Therapy with Immunotherapy
After identifying the resistance mechanism, the researchers explored potential therapeutic interventions.
The study demonstrated that erdafitinib, a selective FGFR inhibitor, can specifically target this pathway and reverse the immunosuppressive effects induced by FGFR3 mutations.
Experimental results showed that erdafitinib can effectively convert the tumor microenvironment from “cold” to “hot” by:
- Reducing the proportion of exhausted T cells
- Increasing infiltration of NK cells
- Increasing infiltration of CD8⁺ cytotoxic T cells
- Enhancing immune-cell activation
- Restoring antitumor immune responses
These findings suggest that FGFR inhibition not only targets tumor cells directly but also remodels the immune microenvironment to become more responsive to immunotherapy.
Erdafitinib Plus PD-1 Blockade Demonstrates Synergistic Antitumor Activity
The researchers further evaluated combination treatment strategies.
Both in vitro and in vivo experiments demonstrated that combining erdafitinib with anti–PD-1 therapy produced synergistic antitumor effects and significantly inhibited tumor growth.
These findings suggest that poor responses to immunotherapy in FGFR3-mutant urothelial carcinoma do not necessarily indicate complete resistance to immune checkpoint inhibition. Instead, targeted intervention may first be required to remodel the tumor microenvironment before immunotherapy can achieve its full therapeutic potential.
In this context, FGFR inhibition may serve as a critical sensitization strategy that enhances responsiveness to PD-1 blockade.
From Clinical Question to Precision Medicine
This study represents a comprehensive research framework that begins with a clinically relevant problem, progresses through mechanistic investigation, and culminates in a potential therapeutic solution.
By leveraging patient-derived organoid models that preserve tumor heterogeneity and immune characteristics, together with multi-omics analyses at single-cell resolution, the investigators successfully linked clinical observations to underlying biological mechanisms.
The findings not only deepen our understanding of immunotherapy resistance in urothelial carcinoma but also provide a compelling rationale for combining targeted therapy and immunotherapy in patients with FGFR3-mutant disease.
As research in this area continues to advance, these insights may pave the way for more personalized and effective treatment strategies for patients with advanced urothelial carcinoma.
Corresponding Authors
Professor Tao Xu
Peking University People’s Hospital
Professor Yihan Lin
Center for Quantitative Biology, Peking University
First Authors

Shan Jiang

Yuxuan Song

Yun Peng