In the evolution of treatment for Multiple Myeloma (MM), moving highly effective therapies forward to the early stages of the disease has become a current research hotspot. For patients with High-Risk Smoldering Multiple Myeloma (HR SMM), whether early active intervention can delay or even prevent its transformation into active myeloma is a focus of clinical attention. At a recent international academic conference, Professor Cyrille Touzeau from the University Hospital of Nantes in France shared the preliminary results of the ERASMM (EMN34) study. This study aimed to evaluate the safety and efficacy of the BCMA×CD3 bispecific antibody Elranatamab in patients with HR SMM. This journal has specially compiled the highlights of the conference for our readers.01 Research Background: Strategy Shift from “Watch and Wait” to “Early Cure”
Smoldering Multiple Myeloma (SMM) serves as an intermediate stage between Monoclonal Gammopathy of Undetermined Significance (MGUS) and active Multiple Myeloma (MM), exhibiting high heterogeneity. In particular, patients with High-Risk Smoldering Multiple Myeloma (HR SMM) face a risk as high as 50% of progressing to active MM within 2 years of diagnosis.
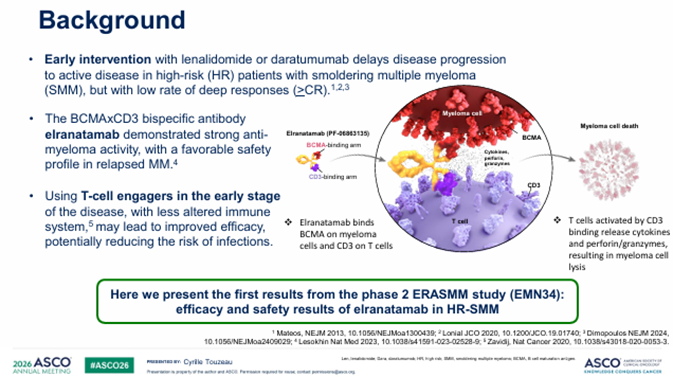
For a long time, the standard management protocol for SMM has been “Watch and Wait.” However, with the emergence of novel immunotherapies, the clinical perspective is undergoing a transformation. Professor Cyrille Touzeau pointed out that in the early stages of the disease, patients’ immune systems are less impaired, and T-cell function is relatively intact. Introducing potent immunotherapies such as T-cell Engagers (TCEs) at this stage could theoretically achieve better immune responses than in the relapsed/refractory stage and potentially reduce the risk of infection. Elranatamab, as a bispecific antibody targeting B-cell maturation antigen (BCMA) and CD3 receptors, has already demonstrated strong activity in Relapsed/Refractory Multiple Myeloma (RRMM). The ERASMM (EMN34) study is based on this background, exploring its potential in early intervention.
02 ERASMM (EMN34) Study Design: Precise Screening and Long-term Management
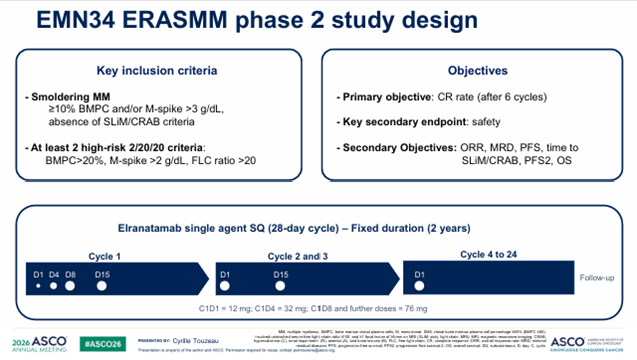
ERASMM is an open-label, multicenter, single-arm, Phase 2 clinical study. The primary objective of the study is to evaluate the efficacy and safety of Elranatamab as a monotherapy in patients with high-risk SMM.
Inclusion Criteria and Risk Stratification: Patients enrolled in the study must meet the diagnosis of HR SMM and exclude SLIM-CRAB criteria (i.e., no evidence of end-organ damage). The determination of high-risk status referred to the International Myeloma Working Group (IMWG) “20/2-20/20” stratification system, which requires meeting at least two of the following indicators:
- Bone Marrow Plasma Cell (BMPC) percentage > 20%;
- Serum Monoclonal Protein (M-protein) > 2 g/dL;
- Involved to uninvolved Serum Free Light Chain ratio (FLCr) > 20.
Dosing Regimen: Patients received a fixed-duration treatment of Elranatamab for two years. To reduce the risk of Cytokine Release Syndrome (CRS), a step-up dosing regimen was adopted in Cycle 1, with priming doses given on Day 1 and Day 4, followed by full doses on Day 8 and Day 15. Cycles 2 to 3 were administered every two weeks (Q2W); from Cycle 4 to Cycle 24 (approximately 2 years), the frequency was adjusted to once a month (Q4W).
Study Endpoints: The primary endpoint was the Complete Response (CR) rate after 6 cycles of treatment. Secondary endpoints included safety, Overall Response Rate (ORR), Minimal Residual Disease (MRD) negativity rate, Progression-Free Survival (PFS), Time to SLIM-CRAB Progression (TTP), and Overall Survival (OS).
03 Patient Baseline Characteristics: High Proportion of Cytogenetic Risk
The study screened 76 patients, and ultimately 50 patients received treatment. The median age was 65 years (range: 42-89 years), with 30% of patients over the age of 70.
Baseline data showed that all patients met at least two IMWG high-risk criteria, with 24% of patients meeting all three criteria simultaneously. Regarding cytogenetics, data were available for 37 patients; according to the latest IMWG 2025 classification, 19% of patients had high-risk cytogenetic features. If a broader definition of high-risk SMM cytogenetics (including t(4;14), t(14;16), 1q gain, and del(13q)) were used, the high-risk proportion was as high as 81%. These baseline characteristics emphasize the high risk of progression in this study population.
04 Safety Analysis: Controllability of CRS and Infection Risk
Compared to its application in the RRMM stage, the safety profile of Elranatamab in the HR SMM population showed an overall controllable and superior trend.
Cytokine Release Syndrome (CRS): The incidence of CRS was approximately 70%, but the vast majority were low-grade. Grade 1 accounted for 46%, Grade 2 for 20%, and only 2 patients (4%) experienced Grade 3 CRS. All CRS events occurred early in treatment and were managed appropriately, with a median duration of only 1 day. No Immune Effector Cell-Associated Neurotoxicity Syndrome (ICANS) was observed during the study.
Notably, a prophylactic Tocilizumab treatment strategy was introduced into the study protocol. Among the 22 patients who received prophylactic medication, the incidence of Grade 1 CRS dropped significantly to 18%, demonstrating the important value of prophylactic intervention in managing TCEs-related toxicities.
Hematologic Toxicity and Infection: The most common hematologic adverse event (AE) was neutropenia, with 40% of patients experiencing Grade 3-4 events. Regarding non-hematologic AEs, the infection rate was 54%, with Grade 3 infections accounting for 14%; no Grade 4 or 5 (fatal) infections occurred. 86% of patients received prophylactic intravenous immunoglobulin (IVIG) replacement therapy, which effectively maintained IgG levels; only 20% of patients had IgG levels lower than 400 mg/dL at any point.
Treatment Discontinuation: Currently, 86% of patients are still receiving treatment. 7 patients discontinued treatment for various reasons, including 5 due to adverse events and 2 due to biochemical progression.
05 Efficacy Results: Deep Remission and Extremely High MRD Negativity Rate
The ERASMM study showed encouraging data in terms of efficacy, reaching the primary endpoint.
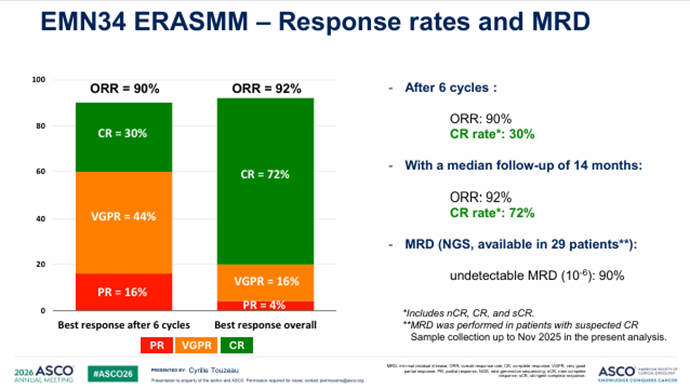
Early Response and Overall Remission: After receiving 6 cycles of treatment, the CR rate reached 30%. As follow-up time extended, the depth of remission continued to deepen. At a median follow-up of 14 months, the ORR was as high as 92%, with the CR rate (including stringent complete response, sCR) significantly increasing to 72%.
MRD Negativity: Among 29 evaluable patients with suspected CR, 90% achieved MRD negativity at the threshold via Next-Generation Sequencing (NGS) testing. This depth of molecular-level remission is rare in previous SMM monotherapy treatments, suggesting that this regimen may bring longer-term clinical benefits.
Survival Benefit: Currently, all patients participating in the study remain alive. The PFS rate is 96%, with only 2 patients experiencing biochemical progression, and no patients have progressed to active MM meeting SLIM-CRAB criteria.
06 Summary and Outlook: Clinical Value of the Immune Front-loading Strategy
Professor Cyrille Touzeau pointed out in the summary that the preliminary results of the ERASMM (EMN34) study confirm the potent activity and good safety tolerability of Elranatamab as an early intervention tool in HR SMM patients.
Core Conclusions:
- Exceptional Efficacy: An ORR of 92% and a CR rate of 72%, combined with a 90% MRD (
) negativity rate, prove that T-cell engagers can exert maximum efficacy in the early stages when the immune system is relatively intact.
- Safety Optimization: Although the incidence of CRS is high, it is mostly Grade 1-2, and the risk can be further reduced through prophylactic use of Tocilizumab; the infection profile is milder than in the RRMM stage.
- Feasibility of Strategy: A fixed two-year treatment cycle not only achieves deep remission but also provides patients with the possibility of a “treatment-free period,” improving quality of life.
In the future, the study will continue follow-up to observe long-term PFS and time to progression. Simultaneously, how to use biomarkers to precisely identify the subgroups that can benefit most from early bispecific antibody intervention will be the direction of further exploration. The success of Elranatamab in HR SMM takes a solid step toward shifting the treatment model of myeloma from “chronic disease management” to “early functional cure.”