
The 18th St.Gallen International Breast Cancer Conference (SGBCC 2023) was held in Vienna, the “World Music Capital,” from March 15 to 18, 2023. SGBCC gathered breast cancer opinion leaders from around the world to discuss and vote on the most cutting-edge and controversial topics in early breast cancer diagnosis and treatment, forming an updated St.Gallen International Expert Consensus on Early Breast Cancer every two years. On the final day of the conference, expert voting took center stage. Oncology Frontier has compiled expert votes on two topics: adjuvant endocrine therapy and chemotherapy decisions for ER-positive breast cancer.
Adjuvant Endocrine Therapy for ER-Positive Breast Cancer
(1) For tumors that are ER low-positive(less than 10%), the appropriate threshold for recommending adjuvant ET is:
1. Any
2. 1%
3. 2%
4. 5%
5. 9%
6. >10%
SGBCC Expert Vote:

(2)Consider a patient with ER positive, HER2 negative breast cancer. The appropriate duration of endocrine therapy for someone with stage 1 disease is:
1. 5 years
2. 7-8 years
3. 10 years
4. Uncertain
5. No adjuvant endocrine therapy
6. Abstain
SGBCC Expert Vote:

(3)Consider a patient with ER positive, HER2 negative breast cancer. The appropriate duration of endocrine therapy for someone with stage 2, node-negative disease is:
1. 5 years
2. 7-8 years
3. 10 years
4. Uncertain
5. Depends on further biological factors
6. Abstain
SGBCC Expert Vote:

(4)Consider a patient with ER positive, HER2 negative breast cancer. The appropriate duration of endocrine therapy for someone with stage 2, node positive disease is:
1. 5 years
2. 7-8 years
3. 10 years
4. Uncertain
5. Abstain
SGBCC Expert Vote:

(5)Consider a patient with ER positive, HER2 negative breast cancer. The appropriate duration of endocrine therapy for someone with stage 3 disease is:
1. 5 years
2. 7-8 years
3. 10 years
4. Uncertain
5. Abstain
SGBCC Expert Vote:

(6) For a patient with stage 2, ER positive, HER2 negative breast cancer, a genomic assay should be used, if readily available, to determine the duration of ET
1. Yes
2. No
3. Abstain
SGBCC Expert Vote:

(7) Adjuvant abemaciclib should be recommended based on tumor stage and histology,irrespective of Ki67 expression,Is this viewpoint correct?
1. Correct
2. Incorrect
3. Abstain
SGBCC Expert Vote:

(8)A patient with ER positive, grade 2 breast cancer has undergone surgery and SLN biopsy for 2.3 cm tumor, with a macrometastasis affecting 1 of 1 SLN. She will get chemotherapy and endocrine therapy. Which of the following would you recommend?
1. No further treatment is needed
2. Axillary lymph node dissection to determine if there are other positive lymph nodes, thereby deciding whether to use abemaciclib
3. Adjuvant abemaciclib therapy
4. Abstain
SGBCC Expert Vote:

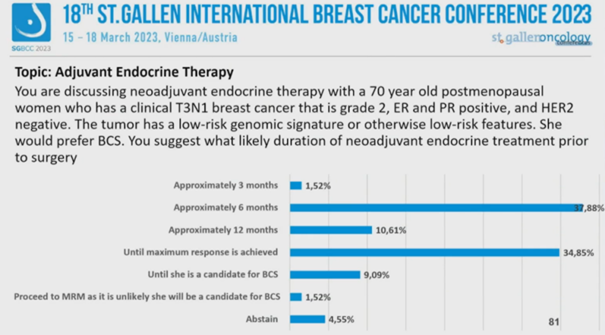
(9)You are discussing neoadjuvant endocrine therapy with a 70 year old postmenopausal women who has a clinical T3N1 breast cancer that is grade 2, ER and PR positive, and HER2negative. The tumor has a low-risk genomic signature or otherwise low-risk features. She would prefer BCS. You suggest what likely duration of neoadjuvant endocrine treatment prior to surgery?
1. Approximately 3 months
2. Approximately 6 months
3. Approximately 12 months
4. Until maximal response is achieved
5. Until BCS eligibility is met
6. Modified radical mastectomy (MRM) due to unsuitability for BCS
7. Abstain
SGBCC Expert Vote:
Chemotherapy Decision for ER-Positive Breast Cancer
(10) Giving a short course of endocrine therapy (2-4 weeks) before surgery, and monitor its effect on Ki67, can provide valuable information for waiving chemotherapy,Is this viewpoint correct?
1. Correct
2. Incorrect
3. Abstain
SGBCC Expert Vote:

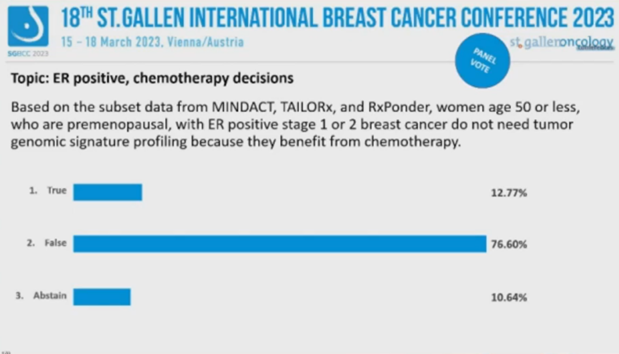
(11) Based on the subset data from MINDACT, TAILORx, and RxPonder, women age 50 or less,who are premenopausal, with ER positive stage 1 or 2 breast cancer do not need tumorgenomic signature profiling because they benefit from chemotherapy.
Is this viewpoint correct?
1. Correct
2. Incorrect
3. Abstain
SGBCC Expert Vote:
(12) A 34 year old premenopausal woman has been diagnosed with a palpable, ER positive, PR positive, HER2 negative breast cancer. The tumor is 1.6 cm, grade 2, and node-negative. The recurrence score is 12. You would recommend:
What do you recommend?
1. Tamoxifen (TAM)
2. Ovarian function suppression (OFS) + TAM
3. OFS + aromatase inhibitor (AI)
4. Sequential chemotherapy followed by endocrine therapy
5. Abstain
SGBCC Expert Vote:

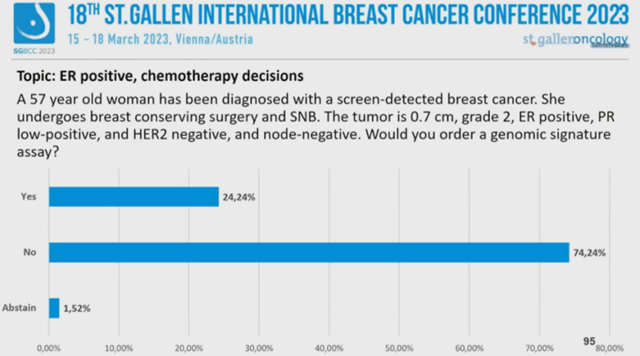
(13) A 57 year old woman has been diagnosed with a screen-detected breast cancer. She undergoes breast conserving surgery and SNB. The tumor is 0.7 cm, grade 2, ER positive, PR low-positive, and HER2 negative, and node-negative. Would you order a genomic signature assay?
1. Yes
2. No
3. Abstain
SGBCC Expert Vote:
(14)A 57 year old woman has been diagnosed with a screen-detected breast cancer. She undergoes breast conserving surgery and SNB. The tumor is 1.7 cm, grade 2, ER positive, PR low-positive, and HER2 negative, and node-negative. She is willing to take chemotherapy ifthere is some benefit. The recurrence score is 26.Would you give chemotherapy?
1. Yes
2. No
3. Abstain
SGBCC Expert Vote:

(15) (Moderator’s spontaneous question) If the patient’s RS is 25, do you recommend chemotherapy?
1. Yes
2. No
3. Abstain
SGBCC Expert Vote:

(16) A 61 year old woman presented with a clinically detected breast cancer and palpable axillary LN.Biopsy confirmed an invasive ductal carcinoma, grade 1, that was strongly ER positive, strongly PR positive, HER2negative cancer, and had a Ki67 below 15%. She underwent mastectomy and axillary node dissection. The primary tumor was 5.1 cm (T3). The recurrence score was 10.
What number of positive axillary lymph nodes would prompt you to recommend ?
1. 2 nodes
2. 3 nodes
3. 4 nodes
4. 8 nodes
5. ≥10 nodes
6. I never recommend chemotherapy in such cases
7. Abstain
SGBCC Expert Vote:

(17) A 57 year old has undergone breast conserving surgery for a stage 1, node negative breast cancer, that is grade 2, ER positive, PR positive, and HER2 negative. She had tumor genomic testing, which shows a high-risk tumor. You would recommend adding chemotherapy to endocrine therapy for a tumor that was which size?
1. 1.5 cm
2. 1.2 cm
3. 1.0 cm
4. 0.8 cm
5. 0.6 cm
6. I never recommend chemotherapy for such stage 1 tumors
7. Abstain
SGBCC Expert Vote:

(18) Patients with invasive lobular breast cancer (grade 1 or 2, strongly ER positive, HER2negative, stage 1-3, and without pleomorphic features) should not receive neo/adjuvant chemotherapy. Is this viewpoint correct?
1. Correct
2. Incorrect
3. Abstain
SGBCC Expert Vote:

(19) Patients with classical invasive lobular breast cancer (grade 1 or 2, strongly ER and PRpositive, Ki67<10%, HER2 negative, and without pleomorphic features), and confirmation of favorable pathology be means of a low genomic signature score, should not receive neo- or adjuvant chemotherapy, if stage 1, 2, or 3. Is this viewpoint correct?
1. Correct
2. Incorrect
3. Abstain
SGBCC Expert Vote:

(20) A 38 year old patient is receiving GnRH agonist and Al therapy for stage 2 breast cancer. She is amenorrheic and experiencing menopausal symptoms. Her monitoring for functional menopause should include:
1. No additional testing
2. Annual monitoring of estradiol levels
3. Monitoring estradiol levels every six months
4. Abstain
SGBCC Expert Vote:

(21) A 39 year old patient is receiving GnRH agonist and Al therapy for stage 2, ER positive, HER2 negative breast cancer. She has breakthrough menstrual bleeding on every 3 month GnRH agonist therapy. You would recommend:
1. Switch to monthly GnRHa
2. Switch to tamoxifen (TAM)
3. Ovarian ablation and continued AI therapy
4. Abstain
SGBCC Expert Vote:

(22)A premenopausal woman in her 40s with stage 3 breast cancer is concluding 5 years of GnRH agonist therapy and paired with a non-steroidal aromatase inhibitor. She has had substantial arthralgias but otherwise found treatment to be acceptable. As ongoing therapy, you would recommend:
1. Discontinue treatment
2. Switch to TAM
3. Switch to GnRHa combined with TAM
4. Continue GnRHa combined with the same AI
5. Continue GnRHa combined with exemestane
6. Abstain
SGBCC Expert Vote:

SGBCC Expert Vote: Which One Would You Choose?
Due to formatting limitations, we have selected 10 questions for readers to vote on, providing a glimpse into the decision-making process for early breast cancer treatment at the St. Gallen International Breast Cancer Conference. The questions are abbreviated, and you can refer to the previous text for their detailed content.
1. ER threshold for adjuvant endocrine therapy (Single choice):
• Any
• 1%
• 2%
• 5%
• 9%
• >10%
2. Duration of adjuvant ET for N+, stage 2 ER+ patients (Single choice):
• 5 years
• 7-8 years
• 10 years
• Uncertain
• Abstain
3. Do stage 2 ER+ patients need genetic testing to determine ET duration? (Single choice):
• Yes
• No
• Abstain
4. Abemaciclib adjuvant therapy can be considered without considering Ki-67 levels (Single choice):
• Correct
• Incorrect
• Abstain
5. Recommendations for adjuvant treatment of ER+, G2, T 2.3cm, 1/1 SLN+ patients (Single choice):
• No further treatment needed
• Axillary lymph node dissection to determine if there are other LN positives, thereby deciding whether to choose abemaciclib
• Abemaciclib adjuvant therapy
• Abstain
6. Giving neoadjuvant ET for 2-4 weeks, monitoring Ki-67 changes to determine neoadjuvant chemotherapy (Single choice):
• Correct
• Incorrect
• Abstain
7. If the patient in question 14 has an RS of 25, would you recommend chemotherapy? (Single choice):
• Yes
• No
• Abstain
8. For gene low-risk (RS 10) patients, how many ALN positives would require chemotherapy? (Single choice):
• 2 nodes
• 3 nodes
• 4 nodes
• 8 nodes
• ≥10 nodes
• I never recommend chemotherapy in such cases
• Abstain
9. For gene high-risk patients, how large should the tumor be to require chemotherapy? (Single choice):
• 1.5 cm
• 1.2 cm
• 1.0 cm
• 0.8 cm
• 0.6 cm
• I never recommend chemotherapy for such stage 1 tumors
• Abstain
10. A 38-year-old patient experiences menopause and menopausal symptoms during ET. What should be monitored? (Single choice):
• No additional testing
• Annual monitoring of estradiol levels
• Monitoring estradiol levels every six months
• Abstain

SGBCC Voting Venue (Photography: Maple Leaf)

